Last year’s flu vaccine was a total bust, yet the CDC claims it was a “grand success” – Here’s the truth of what happened
05/14/2018 / By Lance D Johnson

The Centers for Disease Control (CDC) claims that last year’s flu vaccine was a “grand success.” Newly appointed CDC director Robert R. Redfield claimed the influenza A and B vaccines were 36 percent effective over 2017-2018 flu season. He tweeted praise on the vaccinated because they “reduced risk of getting sick with the flu and having to go to the doctor by about one-third.”
Even though 36 percent effectiveness is scant and meaningless for a product that promises protection against serious disease, this number is NOT based on absolute risk reduction (ARR). Instead, the CDC bases its vaccine effectiveness numbers on something called relative risk reduction (RRR), a vague and misleading postulation that exaggerates the vaccine’s effectiveness. Their numbers are then echoed by the mainstream media to hide the real failure of the flu vaccine.
A more accurate figure for vaccine efficacy can be calculated by configuring the absolute risk reduction. This figure, which we will calculate below, is only about one percent. On top of misrepresenting the data, the CDC omits five other important factors that should be considered in determining vaccine effectiveness, including genetic mutations of flu viruses in vaccines, the shedding of flu viruses from vaccines, weakened humoral immunity after vaccination, the importance of the individual’s terrain in determining outcomes, and vaccine side effects, which can cause flu like illnesses, secondary infections, and neurological events. As we will explore, there is no reliable evidence linking flu vaccination to a flu reduction in the population. The shot actually causes harm to the vaccine recipient and is prone to shedding, increasing the likelihood that more people will become infected with mutated live virus strains.
Calculating absolute risk reduction instead of relative risk reduction
Former CDC director Tom Friedman claimed the vaccine was 60 percent effective last year, but what statistical analysis are these health authorities deriving their conclusions from? Let’s take a closer look: On the surface it sounds like sixty out of one hundred people will benefit from the flu vaccine. According to the current CDC director, it sounds like one in three people will be protected if they just get their yearly flu shot. These numbers, sadly low, are made more preposterous because they are based on the RRR statistical lie.
Here’s how the CDC comes up with the 60 percent effectiveness RRR statistical lie: When 100 unvaccinated people are exposed to the influenza virus, they found that five become ill. Therefore, 95 percent of the people did not get the flu, resulting in 5 percent incidence. If another 100 people got the flu shot and three came down with the flu, then 97 percent of the vaccinated group are declared protected by the vaccines, with a three percent incidence. Under the CDC’s RRR statistical rules, they divide three percent incidence by five percent incidence to get a relative effective rate of 60 percent.
If the CDC followed the more truthful ARR statistical rules, they would divide 95 percent by 97 percent to obtain a more accurate figure of roughly one percent. This means that one hundred people will have to be vaccinated in order for one person to benefit. Even this meager benefit of one percent is ultimately negated due to the fact that 100 percent of all vaccine recipients burden their body with toxins and mutated virus strains that weaken their humoral immune system and cause flu-like symptoms.
Selecting the virus strains for the vaccines is guesswork from the start
It takes at least six months for vaccine manufacturers to bring flu vaccines to market, in anticipation for another flu season. The experts select three or four influenza viruses from the southern hemisphere out of hundreds of different types and mutated subtypes that could circulate the following year in the northern hemisphere. This guesswork makes flu vaccines ineffective from the start.
Researchers find out that flu virus strains quickly mutate in chicken eggs
In order to obtain enough pathological material for widespread vaccine manufacture, scientists must grow the viruses in a medium; however, the viruses adapt to that environment and mutate into new forms. The virus’s genetics change. The viruses that are grown for vaccines are not always the same viruses that are circulating in the wild. This is why the vaccinated are unable to adapt to the pathogens that circulate year to year. The immune systems of the vaccinated are being trained to recognize and respond to viruses that are much different, thereby burdening the vaccinated person’s immune system, distracting immune-responsive cells, and taking away their ability to recognize and face the pathogens that are circulating among them naturally in real time.
Scientists at The Scripps Research Institute (TSRI) found that the practice of growing influenza vaccine components in chicken eggs disrupts the major antibody target site on the virus surface, rendering the flu vaccine less effective in humans. The influenza subtype used in their study, H3N2, quickly mutated when grown in the chicken eggs. By the time the vaccine was put in the marketplace, the viruses people are inundated with do not resemble what they will have to face in real time. Flu vaccines are actually equipping flu viruses with new traits for survival, making flu viruses more diverse, with stronger mutations that can hinder the elderly, the young, and the immunocompromised. This is why many vaccinated individuals tend to get sick three or more times a year. First they may come down with symptoms from the mutated strains, and then they may become ill with the side effects of the vaccine toxins. As their bodies become immunocompromised, they are more susceptible to secondary respiratory infections such as bronchitis and harsh colds. By the time they have recovered, their bodies aren’t prepared to face the actual flu viruses that are circulating in the wild.
Vaccine effectiveness rate does not incorporate any measurement of an individual’s cellular terrain for its potential for harboring or detracting disease
The effectiveness rate of the vaccine is a lie from the start because it only focuses on infection of the germ and not on the status of an individual’s cellular terrain, which can either harbor disease or detract it. In their quests for survival and replication, viruses encounter different cellular and microbial terrains within people. These terrains are formed through dietary choices and are affected by environmental toxins. These terrains vary from person to person, depending on what nutrients they are absorbing and the abundance of healthy microbes that are present inside and outside their bodies.
Viruses encounter different terrains per individual. For example, a flu subtype may cross paths with someone who is chronically deficient in vitamin C, D, magnesium and zinc. The person’s cellular terrain may be functioning at a minimum, their microbiome not processing nutrients due to exposure to antibiotics and antacid drugs. Their weak internal terrain or damaged mucosal membranes may readily harbor disease; whereas, someone who is actively absorbing nutrients may easily repel the same virus material.
Individuals who want to have better outcomes in the face of germs should focus less on the anxiety and fear of infection, and be more focused on empowering the internal terrain of their microbiome and cellular energy production. This strengthening of the terrain is made possible through the absorption of nutritive compounds that benefit immune response, including the utilization of the sun’s energy for vitamin D production. This strengthening is made possible through absorption of the antioxidants and minerals found in plants, the utilization of healthy fats for creating strong cell membranes, and the strengthening and diversifying of healthy microbes in the gut for efficient use of nutrients, blood protection, and stress management. If the CDC wants to prevent flu in the population, they should interview the unvaccinated who rarely get sick and see what they are doing to establish a healthy terrain. (Related: Flu vaccine virtually worthless in people 65 and older: Here’s what you can do instead.)
The reality of virus shedding from attenuated live virus vaccines
If you are afraid of getting the flu and think a vaccine is the best way to protect yourself and those who are immunocompromised – think again. After you are injected with a live attenuated virus, you are 6.3 times more likely to spread the flu virus through the air than your unvaccinated counterparts. A groundbreaking study published in the Proceedings of the National Academy of Sciences (PNAS) debunks herd immunity and actually shows that the vaccinated herd members are the ones perpetuating the disease they were vaccinated for. You may think the unvaccinated are putting the vulnerable at risk, but they aren’t infected by default. They aren’t the ones knowingly becoming 630 percent more likely to spread the flu to the immunocompromised. Live virus shedding after vaccination can occur for several weeks. Those who are vaccinated with live virus vaccines should be quarantined from the young and elderly because they are highly infectious when compared to the unvaccinated who are not carriers of disease by default.
Do flu vaccines cause higher incidence of other infections?
The CDC’s vaccine effectiveness propaganda does not include any mention of secondary respiratory infection, such as severe colds and bronchitis, which are prevalent in the vaccinated. These health issues can cause visits to the doctor just the same. The flu vaccine gives people a false sense of safety, making the vaccinated less likely to take other preventative steps, such as fortifying their body with the right nutrients for a stronger cellular terrain. This would make the vaccinated, in general, more susceptible to secondary infections.
The vaccinated should not just trust in the vaccine to take care of their yearly immunity. As their immune system is burdened with mutated influenza viruses from the vaccine, it is not prepared to handle the viruses that are actually circulating in the wild. Those who choose not to vaccinate are not burdened by mutated pathogens and are more likely to be diligent in fortifying their bodies with the nutrients that strengthen their natural immune response. In this way, the unvaccinated will be more adapted to handle the viruses that they encounter naturally.
Side effects of vaccines burden vaccine recipients, weakening humoral immunity
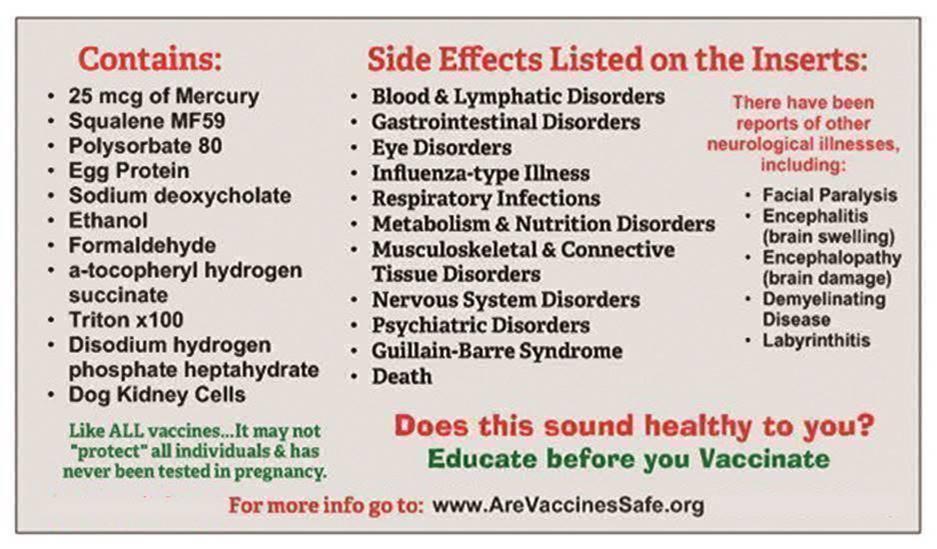
Because the flu vaccine contains mercury, formaldehyde, squalene, Polysorbate 80, and the kidney cells of dogs, the total formula can cause health issues within the body, depending on one’s current health situation. How a person reacts to a vaccine depends on pre-existing conditions such as the state of their microbiome, the health of their kidneys, liver, and lymph, their previous exposure to vaccine toxins and environmental toxins, and the blood to weight volume of the individual being vaccinated. In trying to protect against the flu, the vaccine can simultaneously cause blood and lymphatic disorders, gastrointestinal distress, nervous system disorders, psychiatric events, metabolism issues, eye disorders, influenza-type illnesses. Some bodies reject the toxins in the vaccine quickly, leading to swelling and mood changes. Some toxins cross the blood-brain barrier, leading to encephalitis (brain swelling), encephalopathy (brain damage), and Guillain-Barre Syndrome, three of the more serious neurological events reported after vaccine use.
Vaccine efficacy never truly established before vaccines are licensed
Vaccine efficacy is never truly established before a vaccine comes to market. Vaccine efficacy in human populations is not rooted in clinical studies measuring its true effectiveness in the field. Vaccines are often approved based on animal studies that show that the vaccine induces an immunological response. A vaccine can be licensed based on the assumption that the animal’s immune response will be replicated in the human body through similar pathways. Even worse, vaccines can be licensed without even this correlation. According to the FDA’s “animal rule” the animal efficacy data of the vaccine may establish that there is a reasonable likelihood that the product would produce clinical benefit in humans, with or without any correlation at all. This means that some vaccines are approved without any scientific conclusion, just an untested hypothesis. This means that vaccines are highly experimental, not based on any short or long term outcomes observed in human participants in clinical settings. All effectiveness rates for vaccines are mere projections and postulations, not grounded in real data. No one knows how long a vaccine’s so-called immunity really lasts or if the same immune response observed in animals actually carries over to humans. To make matters worse, the immune response used to license vaccines is based on serology studies. This means that vaccine efficacy is determined by identifying and measuring antibodies in body fluids. This is why adjuvants such as aluminum salts or squalene are added to vaccines, to inflame the injection site and enhance the immune response, to make the vaccine appear more clinically effective. However, the measurement of an immune response in serum is not the same as the true measurement of long term, learned immunity to pathogens of various subtypes and serotypes in the individual.
Did last year’s flu vaccine cause more hospitalizations than it prevented?
The handful of viruses chosen for each year’s flu vaccine is guesswork because there are up to 200 different subtypes of the flu virus that can cause illness and these strains are constantly mutating. After these guesswork viruses mutate in the chicken embryo medium, they do not resemble the actual flu viruses that will circulate among the population. Therefore, getting a flu vaccine is virtually 100 percent useless, with a degree of harm imposed on the vaccine recipient. Nevertheless, in the vaccinated, there is potential for further harm, including the weakening of the individual immune system which becomes mal-adapted to fight future infections. Also, with the vaccinated, the potential for infections to spread are greater, especially in those who are exposed to the aerosolized live virus shedding which comes from the very breath of those vaccinated with live virus strains.
It’s a shame that health care institutions require a defective and harmful product to be mandated on their workers. It’s morally disturbing that this product is marketed to pregnant women and babies.
For more truthful analysis of the flu and other vaccines, visit Vaccines.News.
Sources include:
Tagged Under: absolute risk reduction, adverse events, animal rule, CDC, dangerous toxins, disease prevention, efficacy rate, Flu vaccine, Genetic Mutations, germ theory, hospitalizations, immunity, secondary infections, skeptics, statistical exaggeration, terrain theory, untested hypothesis, vaccine damage, vaccine industry, vaccine licensure, virus shedding

















{kind=link}